What is the choroid?
The Choroid, also known as the choroidea or choroid coat, is the vascular layer of the eye, containing connective tissues, and lying between the retina and the sclera.
What is the histology of the choroid plexus?
Histology of the Choroid Plexus. As mentioned above, if we were to look closely at the medial wall of the lateral ventricle or the roof of the third or fourth ventricle, small invaginations would be visible. The regions of the ventricles that contain invaginations of the pia mater are known as tela choroidea.
Is the choroid part of the uvea?
Choroid anatomy The choroid is part of the uvea, which also consists of the iris and the ciliary body. The iris and ciliary body are located in the front of the eye and work together to dilate and constrict the pupils.
What are the four layers of the choroid?
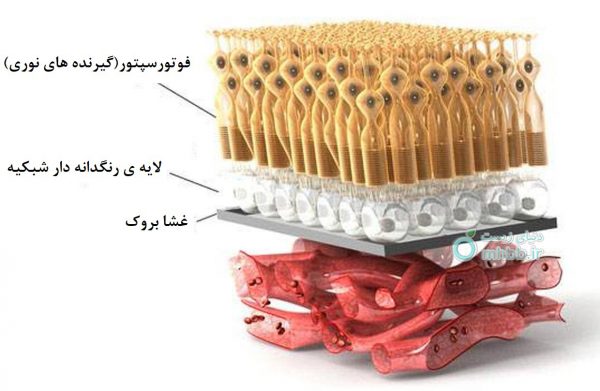
The structure of the choroid is generally divided into four layers (classified in order of furthest away from the retina to closest): Bruch's membrane (synonyms: Lamina basalis, Complexus basalis, Lamina vitra) - innermost layer of the choroid.
Where is the choroid located?
The choroid provides oxygen and nourishment to the outer layers of the retina. Along with the ciliary body and iris, the choroid forms the uveal tract .
How many layers are there in the choroid?
The structure of the choroid is generally divided into four layers (classified in order of furthest away from the retina to closest): Haller's layer - outermost layer of the choroid consisting of larger diameter blood vessels; Sattler's layer - layer of medium diameter blood vessels; Choriocapillaris - layer of capillaries; and.
What is the choroid in the eye?
(Choroid labeled at right, second from the bottom.) The choroid, also known as the choroidea or choroid coat, is the vascular layer of the eye, containing connective tissues, and lying between the retina and the sclera.
Which layer of the choroid contains large blood vessels?
Choriocapillaris – Layer made up of capillaries (tiny blood vessels that connect arteries to veins). Sattler’s layer – Layer of medium blood vessels. Haller’s layer – Outermost layer of the choroid that contains large blood vessels.
How thick is the choroid?
The thickness of the choroid varies depending on what part of the eye it’s lining. For example, it’s the thickest in the back of the eye (approximately 0.2 mm) and narrows to approximately 0.1mm as it gets to the peripheral part of the eyeball. There are four different layers of the choroid:
What is the choroid of the eye?
Choroid of the eye: Anatomy and function. The choroid is the middle layer of tissue in the wall of the eye. It’s found between the sclera (the whites of the eyes) and the retina (the light-sensitive tissue in the back of the eye). This thin layer of tissue is made up almost entirely of blood vessels. These blood vessels supply oxygen and nutrients ...
What is a choroidal rupture?
Choroidal rupture – A tear in the choroid, Bruch’s membrane and the retinal pigment epithelium (RPE) that result from an eye injury. Choroid plexus papilloma – Rare, benign brain tumor that develops in the choroid plexus (tissue that makes cerebrospinal fluid).
What is the term for inflammation of the choroid?
Chorioretinitis – Inflammation of the choroid caused by infection or an autoimmune disease. Choroideremia – A hereditary, progressive deterioration of the choroid; this condition primarily affects men.
What is the term for a tear in the choroid?
Choroidal detachment and hemorrhage – Separation of the choroid from the sclera; this may happen as a result of low eye pressure (serous choroidopathy, which is fluid-filled) or high eye pressure (hemorrhagic choroidopathy, which is blood-filled). Choroidal rupture – A tear in the choroid, Bruch’s membrane and the retinal pigment epithelium (RPE) ...
What is the function of the choroidal circulation?
Choroidal circulation accounts for 85% of blood flow within the eye, making it a vital structure to the function of your eyes.
Where is the choroid plexus located?
The cerebral aqueduct is void of choroid plexus. The choroid plexus is located in the posterior medullary velum which partially forms the roof of the fourth ventricle.
When does the choroid plexus develop?
Signs of choroid plexus development of the fourth ventricle are evident around the 6th or 7th week of gestation , with the choroid plexus of the lateral ventricles developing at the same time, or shortly after in week 7. The choroid plexus of the third ventricle generally begins to develop a bit later in week 8.
What is the most common treatment for choroid plexus papilloma?
A solid mass, with some calcifications, is generally evident on imaging. The most common treatment for choroid plexus papilloma is complete surgical excision.
What type of cell is the choroid plexus?
a fourth ventricle. These ventricles are lined by a specialized type of glial cell called ependymal cells, or the ependyma. The choroid plexus is formed by these vascularized invaginations, bordered by the ependyma.
Where do the endothelial cells of the choroid plexus come from?
However, the endothelial cells of all the choroid plexuses, and the mesenchymal stem cells (cells that differentiate into other cell types) of the choroid plexus of the fourth ventricle are derived from the cephalic mesoderm.
Which region of the ventricles contains invaginations of the pia mater?
The regions of the ventricles that contain invaginations of the pia mater are known as tela choroidea. The deepest component of the choroid plexus is a layer of simple cuboidal epithelial cells, collectively known as the ependyma. This ependymal layer, with hair like projections, is composed of ependymal cells.
Which artery supplies the choroid plexus?
The choroid plexus of the lateral ventricles are supplied by the anterior choroidal arteries (branch of internal carotid artery) and the lateral posterior choroidal arteries (branch of the posterior cerebral artery ). Anterior choroidal artery (caudal view)
Choroid Structure
Haller’s layer – outermost layer of the choroid, comprising large diameter blood vessels
Choroid Anatomy
This structure covers to the interior the fibrous eye’s tunic. It makes up the posterior part of the uvea, the anterior is indicated by a thick area, the ciliary zone. The two areas are discriminated by the ora serrata at the eye’s equator, which is formed as a scalloped line.
Function of Choroid
For the proper functioning of the eyes and for a clear vision, it is vital to be supplied with adequate blood supply. The choroidal circulation is said to be responsible for about 85% of the blood flow in the eye, thus making it an important structure to the function of eyes. Some other functions are –
Choroid Eye Conditions
There are several reasons which can cause the choroid to develop certain conditions, such as genetic, sporadic or even trauma to the eye. Following are the conditions which could affect the choroid –
Summary
Choroid forms a vital structure of the eye which could be included in several pathologies. It is of immense significance provided its functions such as thermoregulation, vascularization and even in the production of the growth factors.
Where does the anterior choroidal artery originate?
It originates from the posterolateral aspect of the internal carotid artery, between the posterior communicating branch (PCOM) and the terminal ICA bifurcation.
How thin is the anterior choroidal artery?
The anterior choroidal artery is very thin in caliber, averaging approximately 0.94 mm in diameter. In addition, its perforating branches have a long course and an extensive supply of various brain structures. Therefore, a stroke (ischemic/hemorrhagic) of the anterior choroidal artery can happen very easily and have life-threatening implications.
What causes choroidal stroke?
The main causes of anterior choroidal strokes are thromboembolisms from the internal carotid artery or small vessel infarcts due to autoimmune conditions (lupus, vasculitis).
What is the preterminal branch of the communicating segment of the internal carotid artery?
The anterior choroidal artery is the preterminal branch of the communicating segment (C7) of the internal carotid artery. It supplies several subcortical structures ( limbic system, basal ganglia, diencephalon ), midbrain, temporal lobe and visual pathway. Therefore, these structures will be the main ones affected during a stroke of the anterior choroidal artery.
What are the symptoms of an anterior choroidal artery stroke?
They can range from lacunar infarct symptoms (hemiparesis, hemiplegia, dysarthria, weakness) to visual field deficits, somnolence, aphasia or neglect. The evolution of such a stroke is also varied.
What are the four parts of the brain that are supplied by the hippocampus?
They supply the amygdala, hippocampus, globus pallidus, substantia nigra, caudate nucleus, hypothalamus, red nucleus, tela choroidea, posterior limb of the internal capsule, optic tract, crus cerebri of the midbrain and fimbria of the fornix.
Where does the intraventricular segment continue?
The intraventricular segment continues within the lateral ventricle, accompanying the choroid plexus. At this point, it receives the lateral posterior choroidal branch of posterior cerebral artery. The segment then continues superiorly around the thalamus, until the interventricular foramen (of Monro).
Popular Posts:
- 1. which institute is best for medical transcription course in bangalore
- 2. what is financial management course
- 3. what is the best lsat prep course to take
- 4. how to write a college course curriculum
- 5. how long is billing and coding course
- 6. how long is medical assistant course
- 7. what is pmp training course
- 8. what is a course management system
- 9. what is business management course
- 10. how long is hvac course