Treatment depends on the type of metastasis and its primary source. Treatment options often include chemotherapy, immunotherapy and radiation therapy. In general, chemotherapy and immunotherapy take a relatively long time to work, whereas radiation therapy is more rapid.
Full Answer
How are ocular metastases treated?
Treatment for ocular metastases requires a tight alliance between ocular and general oncologists. If a metastasis is the first indication of a systemic cancer—as it often is with lung cancer—the ocular oncologist may refer the patient to a general oncologist and advise the clinician about the type of tumor to look for.
When should you see an ophthalmologist for ocular metastases?
Detection of a suspected ocular metastasis should prompt an immediate referral to an ocular oncologist or, if that individual is not available, to a retinal specialist. “The referring ophthalmologist doesn’t even have to be right about the diagnosis,” Dr. Murray said. “If they even think it’s a cancer, we’ll see the patient right away.
What are the signs and symptoms of ocular metastases?
Not all ocular metastases fit the classic presentation of a creamy yellow mass deep to the retina. Less common presentations include a serous, nonrhegmatogenous retinal detachment with no apparent mass (flat metastasis), a swollen optic disc (optic nerve metastasis) or a hypopyon to the anterior chamber.
What is included in patient history for ocular metastasis?
In that most patients with ocular metastasis have either a known primary cancer and/or metastatic tumors in other parts of their body; a careful medical history is important. Patients know of prior cancer history and many can remember their tumor stage. History taking can also uncover the signs or symptoms of these other cancers.
What is the life expectancy of someone with metastatic ocular melanoma?
The 5-year survival rate for eye melanoma is 82%. When melanoma does not spread outside the eye, the 5-year relative survival rate is about 85%. The 5-year survival rate for those with disease that has spread to surrounding tissues or organs and/or the regional lymph nodes is 71%.
Is ocular cancer treatable?
Eye cancer is most treatable when it is discovered early, says Renelle Lim, MD, a Yale Medicine ophthalmologist and specialist in ocular oncology and plastic surgery. “For that reason, we always advise everyone to have a dilated eye exam once a year with an eye doctor,” she says.
What is the most common type of cancer to metastasize to the eye?
The most common sources of ocular metastasis are breast cancer (primarily in women) followed by lung cancer (more commonly in men). However, other less common sources include gastrointestinal, prostate, lymphoid, leukemia, thyroid, kidney and skin (primarily melanoma).
What is the best treatment for ocular melanoma?
Surgery. Surgery is the most common treatment for intraocular melanoma. The following types of surgery may be used: Resection: Surgery to remove the tumor and a small amount of healthy tissue around it.
Does eye cancer spread to the brain?
In addition to damaging vision, eye tumors can spread to the optic nerve, the brain and the rest of the body. Therefore, early diagnosis and treatment are extremely important.
What are the side effects of radiation treatment in the eye?
Possible side effects of radiation therapy The main concern with radiation therapy is damage to parts of the eye, leading to problems such as blurry vision, dry eye, cataracts, retinal detachment, glaucoma (increased pressure inside the eye), loss of eye lashes, problems with tear ducts, or bleeding into the eye.
How do you know if cancer has spread to your eye?
How does the doctor know I have eye cancer? Some signs of eye cancer are vision changes (things look blurry or you suddenly can't see), floaters (seeing spots or squiggles), flashes of light, a growing dark spot on the iris, change in the size or shape of the pupil, and eye redness or swelling.
When does cancer spread to the eye?
OCULAR MANIFESTATIONS The principal indication of metastatic carcinoma is blurred or distorted vision in one or both eyes. Usually, the pain is not a sign of metastatic cancer to the eye, except cases that patients have an extensive intraocular tumor.
What is Orbital metastasis?
Several types of cancer can spread (metastasize) to reach the tissues around the eye (orbit). The most common orbital metastases are cancers of the breast, lung, kidney or prostate gland. About 20% of patients who present with an orbital metastasis do not have a known primary cancer elsewhere.
Does Immunotherapy work for ocular melanoma?
An investigational immunotherapy drug has helped patients with uveal melanoma, an aggressive cancer of the eye, live longer than other patients who received current treatments for the disease, according to the results of a large clinical trial.
Is ocular melanoma treatable?
These rare cancers can be treated with either surgical removal of the tumor, if it is small enough, or radiation therapy. In more advanced cases or if there is serious eye damage, enucleation (removal of the eyeball) may be needed.
What happens when ocular melanoma spreads to the liver?
Uveal melanoma, the most common primary intraocular tumor,1–4 has an associated approximate 40% risk of metastasizing to the liver within 10 years of diagnosis of the primary tumor. Hepatic metastases, which occur in 95% of patients with metastatic uveal melanoma,5 result in death in almost all cases.
What to do if you suspect ocular metastasis?
Referral. Detection of a suspected ocular metastasis should prompt an immediate referral to an ocular oncologist or, if that individual is not available, to a retinal specialist. “The referring ophthalmologist doesn’t even have to be right about the diagnosis,” Dr. Murray said. “If they even think it’s a cancer, we’ll see the patient right away. We never say no to a patient.”
What kind of oncologist treats ocular metastases?
Treatment for ocular metastases requires a tight alliance between ocular and general oncologists. If a metastasis is the first indication of a systemic cancer—as it often is with lung cancer—the ocular oncologist may refer the patient to a general oncologist and advise the clinician about the type of tumor to look for. For patients with previously treated cancers, the ocular oncologist may begin the restaging process and, if necessary, treat the ocular metastasis while referring the patient back to the general oncologist.
Why is ocular ultrasound important for metastases?
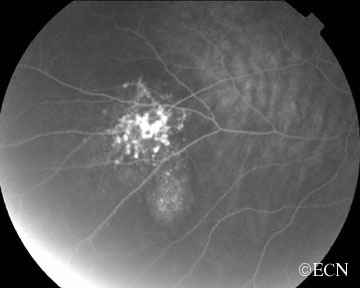
Dr. Shields agreed. “Ocular ultrasound is really important with metastases because they tend to be echogenic, whereas melanoma tends to be echolucent. A fluorescein angiogram also is useful because metastases tend to be hypofluorescent in the early angiogram and later show diffuse patchy fluorescence with multifocal leaks in the RPE. It’s those leaks that lead to retinal detachment.” Optical coherence tomography, she added, will help determine if subretinal fluid is present and is a good way to follow these lesions. Fine-needle aspiration biopsy is reserved for patients who have a negative preliminary workup and is necessary for only 1 to 2 percent of her patients.
What is the role of an ocular oncologist?
The ocular oncologist also may play a role in monitoring the patient’s systemic therapy. “General oncologists love to have us see their patients because the eye is one of the few sites where you can actually see a metastasis and watch it respond to therapy,” noted Dr. Shields. “If a patient has a choroidal metastasis, we measure it and document it with photography. The general oncologist then gives the chemotherapy or hormone therapy and sends the patient back to us two months later and say, 'How are we doing?'”
How thick is a breast metastasis?
According to Dr. Shields, breast cancer metastases tend not to be very thick, measuring about 2 to 3 millimeters, vs. an average thickness of 5.5 mm for melanoma. Metastases also tend to be yellow and very homogeneous in appearance, and the overlying retinal pigment epithelium is not as disturbed as it often is with a melanoma.
How many cases of eye cancer are there per year?
These are the most common ocular malignancies, with an estimated incidence of 30,000 cases per year (vs. about 2,500 cases of primary eye cancers). But many eye metastases go unrecognized.
What is the treatment for asymptomatic eye cancer?
If their systemic disease is out of control, these patients will be treated by their general oncologist. “But if the tumor is threatening vision, we’ll institute radiation therapy ,” said Dr. Murray. “We use external beam radiation if there is multifocal involvement in one or both eyes. If there is only one tumor, the alternative is to do plaque radiotherapy ."
What is the best treatment for radiation blepharitis?
Radiation blepharitis (eyelid inflammation) can be treated with silvadine ointment, black tea soaks, or A&D ointment. If not already working with one, patients are strongly encouraged to consult with an oncologist to construct a proper surveillance schedule for ongoing observation and care.
What is the term for the removal of the eye?
Transretinal endoresection. Enucleation . Enucleation refers to full removal of the affected eye. After enucleation surgery, the patient is admitted to the hospital and the eye is removed under either local or general anesthesia. The enucleated eye cannot be treated or repaired and replaced in the eye socket.
How long after cataract surgery can you go home?
The patient usually leaves the hospital one or two days after surgery. In some cases, patients are permitted to go home the same day. Three to six weeks later, a specialist who makes artificial eyes (called an ocularist) fits the patient with a prosthesis.
What is a partial choroidectomy?
Transscleral partial choroidectomy (cyclochoroidectomy) – A viable therapeutic option for the subset of patients with choroidal or ciliochoroidal tumors who are poor candidates for radiotherapy but are highly motivated to avoid enucleation ( http://archopht.ama-assn.org/cgi/content/full/120/12/1659)
What is the most common form of radiation treatment?
Brachytherapy ("Plaque Therapy") Also known as sealed source radiotherapy or endocurietherapy, brachytherapy is the most common form of radiation treatment. With plaque therapy, a small disc-shaped shield known as a plaque encasing radioactive seeds (most often Iodine-125, though Ruthenium-106 and Palladium-103 can also be used) ...
Can an enucleated eye be repaired?
The enucleated eye cannot be treated or repaired and replaced in the eye socket. Instead, it is replaced with a ball implant that may be made of plastic, a porous material called hydroxylapatite, or other materials. The implant is sewn into position and the eye is allowed to heal.
Abstract
AIMS Three issues were investigated in adult outpatients with orbital metastases. One, how accurate are current diagnostic methods? Two, what is the survival associated with orbital metastases? Three, did any clinical factors correlate with prognosis in this patient cohort?
Methods
We retrospectively reviewed the ocular oncology database at the University of California, San Francisco, for outpatients managed from 1976 to 1995 in whom the diagnosis of orbital metastases was established. Hospitalised patients with widespread disease, noted to have incidental orbital metastases, were excluded from this analysis.
Results
There were 15 males and 16 females, with a median age of 57 years (range 37 to 77 years). The racial distribution was five black, one Asian, and 25 white patients.
Discussion
Orbital metastases are relatively uncommon. In our experience 36 of 612 orbital biopsies for suspected neoplasm (6%) were metastatic in origin; this incidence is similar to that reported in other series.
Acknowledgments
This study was performed at the Department of Ophthalmology, University of California, San Francisco, USA. It was supported in part by That Man May See, San Francisco, California, USA.
Request Permissions
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
Treatment Options
The liver is (initially) the exclusive site of choroidal melanoma metastasis in about 40% of patients. Of those patients, most have diffuse or multi-focal tumors which cannot be removed. Treatment options depend on the size, location and rate of tumor growth.
Observation
It is a patient’s right to choose or refuse treatment. Since many of the previously mentioned treatments can decrease a patient’s quality of life, each decision to treat must be weighed against potential side effects.
Where is the radiation placed in the eye?
In this type of radiation treatment, radioactive material is surgically placed on the outside wall of the eye, in the same spot that the tumor is on the inside of the eye. Our experts have decades of experience using brachytherapy for eye melanoma, and we treat many people with this approach.
How many cases of melanoma are there in MSK?
At MSK, we see more than 200 cases of benign eye lesions (choroidal nevi) each year and treat approximately 60 people with new eye melanomas (also called ocular melanoma) each year.
Can you have an eye melanoma removed?
Depending on the size, location, and stage of the tumor, we may recommend that you have an operation to remove the eye. We often suggest this approach, called enucleation, if you have a relatively large eye melanoma. If the tumor is small, we may be able to treat it effectively with laser therapy.
Is MSK effective for a tumor?
Clinical trials sponsored by the National Institutes of Health, in which MSK played a leadership role, have proven that the removal of the eye and brachytherapy are equally effective for survival in people with medium-size tumors.
How many procedures are performed for metastatic melanoma?
We perform more than 350 procedures annually for patients with metastatic uveal (ocular) melanoma. The course of treatment for this disease is generally determined by progression of the disease in the liver. There are currently no effective systemic chemotherapy regimens for treatment of liver metastases from this tumor.
How long does it take to recover from a liver metastasis?
This procedure improves survival for those with liver metastases from, at best, five months under conventional treatment to an average of 14.5 months. There are just a few other centers in the country that treat uveal (ocular) melanoma, and none through immunoembolization.
What is the treatment for liver tumors?
Chemoembolization is performed in patients with more extensive tumor involvement in the liver. BCNU (a chemotherapy drug) dissolved in an oily liquid (Ethiodol) is injected directly into the arteries supplying the liver, along with a temporary dissolvable agent (Gelfoam) to block off the blood supply to the tumors.
What is the best way to receive new treatments?
Clinical trials are the best way patients can receive new therapies and procedures. To find out if a clinical trial might be right for you, ask your health care provider or contact the Sidney Kimmel Cancer Center Clinical Research Management Office at 215-955-1661.
What is the treatment for metastasis?
Treatment depends on the type of metastasis and its primary source. Treatment options often include chemotherapy, immunotherapy and radiation therapy. In general, chemotherapy and immunotherapy take a relatively long time to work, whereas radiation therapy is more rapid. The choice of chemotherapy , immunotherapy or radiation therapy typically depends on the type of tumor and the temporal “timing” risk for loss of vision.
What cancers can be metastasized to the eye?
Ocular or eye metastasis are usually from a breast cancer (in women) and lung cancer (in men). Other less common sites of origin include the prostate, the kidney, the thyroid, and gastrointestinal tract. Blood cell cancer (lymphoma and leukemia) can also metastasize into the eye and orbit. In 18% of patients, the primary source ...
What is choroidal metastasis?
Treatments. After irradiation, a regressed choroidal metastasis displays spicular hypertrophy of the retinal pigment epithelium. Most patients with ocular metastasis have either a known primary cancer and/or metastatic tumors in other parts of their body.
Can choroidal metastasis be seen in the eye?
As stated, most patients with choroidal metastasis have no symptoms. However, if the metastasis is on the eye or eyelids, it may be visible. If the metastasis is located behind the eye (in the orbit), the eyeball may be visibly displaced out or to the side. If the metastasis is within the eye (the most common), metastasis patients can can have symptoms of flashing lights, floating spots or distortion of their vision. In that waiting until patients are symptomatic may be too late to preserve vision, Dr. Finger suggests that all patients with a history of metastatic cancer should have periodic eye examinations.
Is ocular metastasis a primary cancer?
In that most patients with ocular metastasis have either a known primary cancer and/or metastatic tumors in other parts of their body; a careful medical history is important. Patients know of prior cancer history and many can remember their tumor stage. History taking can also uncover the signs or symptoms of these other cancers.
Can intraocular cancer go undetected?
Though they are the most common intraocular cancer in adults, they usually go undetected. This is because most ocular metastases go undetected unless they affect vision, are visible to the patient, or push the eye forward. Eye metastasis are most commonly found in the vascular choroid (choroidal metastasis) within the eye.
Can lymphoma be metastasized to the eye?
Blood cell cancer (lymphoma and leukemia) can also metastasize into the eye and orbit. In 18% of patients, the primary source of the metastasis may be undetectable. In these cases, Dr. Finger may have to biopsy the ocular tumor to obtain tissue for pathology (to determine the primary source).
How to treat melanoma in the eye?
Treatment for ocular melanoma may include one or more of the following: Surgery. Iridectomy: Removal of part of the iris. Iridotrabeculectomy: Removal of part of the iris, plus a small piece of the outer part of the eyeball. Iridocyclectomy: Removal of a portion of the iris and the ciliary body.
What is the procedure for removing a melanoma?
Transscleral resection: Surgical removal of just a melanoma of the ciliary body or choroid. Enucleation: Removal of the entire eyeball. Orbital exenteration: Removal of the eyeball and some surrounding structures such as parts of the eyelid and muscles, nerves, and other tissues inside the eye socket.
What is the most common eye cancer?
Eye cancer occurs when cells in the eye grow out of control. The most common type of eye cancer is intraocular melanoma, though it’s still a fairly rare type of cancer . Ocular melanoma usually develops in the uvea (uveal melanomas) and rarely in the conjunctiva (conjunctival melanomas).
What type of radiation is used to treat melanoma?
Proton beam radiation therapy. Stereotactic radiosurgery. Laser therapy. Transpupillary thermotherapy (TTT) is the most common type of laser treatment for eye melanoma that uses infrared light to heat and kill the tumor.
How much cancer spreads outside the eye?
Localized (no sign the cancer has spread outside the eye): 85% . Regional (cancer has spread outside the eye to nearby structures or lymph nodes ): 71%. Distant (cancer has spread to distant parts of the body such as the liver): 13%.
What is a dark spot on the eye?
A growing dark spot on the colored part of the eye ( iris) Change in size or shape of the pupil. Change in position of the eyeball within the socket. Bulging eye. Change in the way the eye moves within the socket. Lump on the eye or in the eyelid that is growing.
What is melanoma in the eye?
Ocular melanoma (melanoma in or around the eye) is a type of cancer that develops in the cells that produce pigment — the substance that gives your skin, hair a. Ocular melanoma (melanoma in or around the eye) is a type of cancer that develops in the cells that produce pigment — the substance that gives your skin, hair and eyes color.
What is the innermost layer of the eye?
The innermost layer is the retina. The middle layer between the sclera and retina is called the uvea. Rarely, eye melanoma can also occur on the conjunctiva. Because most eye melanomas form in the part of the eye you can’t see when looking in a mirror, they can be difficult to detect.
Can melanoma be found in the eye?
Just as you can develop melanoma on your skin, you can also develop it inside your eye or on your conjunctiva. Although it is the most common eye cancer in adults, ocular melanoma is very rare. Ocular melanomas usually begin in the middle of the three layers of your eye. The outer layer of your eye is the sclera.
Popular Posts:
- 1. which institute is best for medical transcription course in bangalore
- 2. what is financial management course
- 3. what is the best lsat prep course to take
- 4. how to write a college course curriculum
- 5. how long is billing and coding course
- 6. how long is medical assistant course
- 7. what is pmp training course
- 8. what is a course management system
- 9. what is business management course
- 10. how long is hvac course